
Kawasaki-like disease in children with COVID-19
- Case Based Review
- Published:
- Volume 40, pages 2105–2115 (2020)
- Cite this article
Abstract
Children with Coronavirus disease 2019 (COVID-19) are being reported to have manifestations of hyperinflammatory states and/or Kawasaki-like disease. In this study, we investigated children with typical and atypical Kawasaki disease (KD) likely to be associated with COVID-19. We have reported four children with Kawasaki-like disease probably associated with COVID-19. The clinical features were consistent with incomplete KD in three patients. SARS-CoV-2 RT-PCR was positive in one and the serology was positive in one patient with negative RT-PCR. Corticosteroids, anakinra, intravenous immunoglobulin (IVIG), and acetylsalicylic acid were used in the treatment. Three patients recovered after the treatment while one patient died. The literature review revealed 36 articles describing 320 children with Kawasaki-like disease associated with COVID-19. SARS-CoV-2 RT-PCR was negative in 120 (65.5%) of 183 patients while the serology was positive in 130 (83.8%) of 155 patients. The therapeutic options have included IVIG, acetylsalicylic acid, tocilizumab, anakinra, enoxaparin, and methylprednisolone. Pediatric COVID-19 cases may present with atypical/incomplete Kawasaki-like disease. Thus, pediatricians need to be aware of such atypical presentations resembling KD for early diagnosis of COVID-19.
Similar content being viewed by others
{kind=link}
{kind=link}
Impact of COVID-19 infection on Kawasaki disease and immune status in children
{kind=link}
Explore related subjects
Discover the latest articles, books and news in related subjects, suggested using machine learning.Introduction
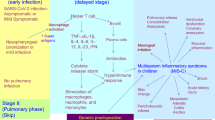
Coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has affected individuals of all ages worldwide. Children constituted only a small proportion of patients with COVID-19, which was initially reported as 1.7% [1]. The actual incidence is unknown since there are no community-based studies. While more than 90% of children with COVID-19 were described to have asymptomatic, mild, or moderate disease, new concerns emerged with reports on hyperinflammatory states or Kawasaki-like disease [2, 3]. The resulting phenotypes are a combination of typical/atypical Kawasaki disease, Kawasaki shock syndrome, toxic shock syndrome, and macrophage activation syndrome/hemophagocytic lymphohistiocytosis [4, 5]. Children with hyperinflammatory syndrome and multiorgan involvement were classified as having pediatric inflammatory multisystem syndrome (PIMS) or multisystem inflammatory syndrome in children (MIS-C) [6, 7].
Kawasaki disease (KD) is an acute, systemic vasculitis of medium-sized vessels. Its etiology has not been clearly elucidated. Infectious triggers have been suggested in the etiology of KD due to having an epidemic pattern and marked seasonality [8]. Various infectious agents, including bacteria such as Streptococcus pyogenes, Staphylococcus aureus, and Yersinia pseudotuberculosis, and viruses such as adenovirus, enteroviruses, Epstein–Barr virus and coronavirus (New Haven coronavirus/HCoVNH) have been implicated in the etiology of KD [9,10,11]. Recently, along with the COVID-19 pandemic, Kawasaki-like disease associated with COVID-19 has been increasingly reported. Large case series of KD related to SARS-CoV-2 from the United Kingdom (UK), Italy, the United States of America (USA), and France were published [6, 12,13,14,15,16,17].
Kawasaki-like disease might be severe and requires more aggressive management. Herein, we report the characteristics of four patients with Kawasaki-like phenotype associated with COVID-19 from Turkey and analyze the features of similar published cases through a systematic literature review. We also discussed the effect of the local characteristics such as the presence of Bacillus Calmette–Guérin (BCG) vaccine in the routine vaccination schedule and high MEFV mutation carriage rate on disease course. Increasing reports of this phenotype from different countries would widen the spectrum of clinical and laboratory features, facilitate the diagnostic process, and provide more clues leading to early and effective treatment.
Search strategy
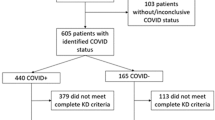
We performed a search through Pubmed/MEDLINE, Scopus and Web of Science databases using the following keywords: “Coronavirus disease-19”, “COVID-19”, “2019 novel coronavirus diseases”, “severe acute respiratory syndrome coronavirus 2”, “SARS-CoV-2”, “2019-nCoV”, “Kawasaki disease”, “incomplete Kawasaki disease”, “atypical Kawasaki disease”, “Kawasaki-like disease”, and “Kawasaki-like syndrome” filtered for articles published in English and Turkish. We searched the literature from inception to August 20, 2020. The systematic review was performed according to the PRISMA checklist (www.prisma-statement.org/. We included all articles that reported children who had Kawasaki-like disease associated with COVID-19. The schematic overview of the literature review process is shown in Fig. 1. The following parameters were noted from included studies: age, gender, country, diagnosis, and diagnostic tests for COVID-19. Diagnosis of complete KD was based on the criteria of the American Heart Association (AHA): the presence of fever for at least 5 days accompanied by the presence of at least four of the following five findings: bilateral non-exudative conjunctival injection, unilateral cervical lymphadenopathy, changes in the lips and oral cavity, skin rash, and changes in extremities, including indurative angioedema and desquamation [18]. Incomplete KD was diagnosed in the presence of unexplained prolonged fever, two or three diagnostic criteria, and supporting compatible laboratory or echocardiography (ECHO) findings [18].
Schematic overview of the studies reporting children with COVID-19-associated Kawasaki-like disease included in the literature research
Case presentations
Case 1 (admission: April 13, 2020)
A 7-year-old boy presented with fever, cough and an erythematous rash. He had bilateral conjunctival injection, diffuse erythematous maculopapular rash, erosive hyperemia of the oral mucosa, bilateral crackles on chest auscultation and respiratory distress findings in physical examination. Respiratory distress developed rapidly, and he was intubated due to hypoxemia. Laboratory tests revealed mild elevation of liver transaminases, lymphopenia, thrombocytopenia, elevated d-dimer, and lactate dehydrogenase levels. His ferritin level was within normal range when he was referred to our hospital on the 12th day of fever, but rose to 1336 µg/L (20–336) on day 27. The SARS-CoV-2 RNA was not detected from his nasopharyngeal swab. However, the bronchoalveolar lavage fluid tested positive for SARS-CoV-2 by real-time reverse transcriptase-polymerase chain reaction (RT-PCR). Chest computed tomography revealed bilateral diffuse ground-glass density areas.
Diffuse enlargement in the left coronary artery (diameter of the left coronary artery was 3.3 mm and Z score 2.0) with normal systolic function and pulmonary hypertension were reported in ECHO findings. The patient was diagnosed with incomplete KD and COVID-19 pneumonia. Intravenous immunoglobulin (IVIG), azithromycin, hydroxychloroquine, ritonavir and lopinavir, tocilizumab, and mesenchymal stem cell treatments were applied during his admission in the pediatric intensive care unit. On the 27th day of the onset of the fever, his hypoxia deteriorated under mechanical ventilation. He was started on venovenous extracorporeal membrane oxygenation (VV-ECMO) therapy. Disseminated intravascular coagulation, renal, and heart failure were developed in the follow-up. He died from severe hypoxia on the 17th day of VV-ECMO.
Case 2 (admission: July 11, 2020)
A 10-year-girl presented with resistant fever for the last 4 days, which was accompanied by vomiting. Physical examination was remarkable with one-sided submandibular lymphadenopathy size of 2 × 1.5 cm, changes in the lips and oral cavity, maculopapular erythema around the neck, bilateral non-exudative conjunctival injection, and diffuse abdominal tenderness. She had prolonged capillary refill time with hypotension. Inotropic therapy was initiated due to hypotensive values resistant to fluid therapy. Her laboratory examination revealed impairment of renal function, high levels of acute phase reactants [C-reactive protein (CRP) 26.4 mg/dl (0–0.8), erythrocyte sedimentation rate (ESR) 96 mm/h (0–20)], lymphopenia with normal leukocyte count, normal platelet levels (155 × 103/µl), elevated brain-natriuretic peptide, d-dimer, ferritin (1019.6 µg/l) and triglyceride levels. Pleural effusion and ground-glass densities were evaluated in favor of COVID-19 in the thoracic tomography of the patient who developed respiratory distress in the follow-up. Besides, an edematous gall bladder was observed on abdominal tomography. She had no contact history for COVID-19, and the RT-PCR test result was negative. She was diagnosed with KD due to the fever and accompanying findings; the conjunctival injection, unilateral cervical lymphadenopathy, changes in the lips and oral cavity, and skin rash. ECHOc was normal. Intravenous immunoglobulin (IVIG), recombinant interleukin 1 (IL-1) receptor antagonist (anakinra), and corticosteroid therapies (20 mg/day) were administered due to the accompanying hyperinflammatory syndrome. The COVID-19 nasopharyngeal swab test result, which was examined for the second time, was negative, while serologic testing for IgG antibodies against SARS-CoV-2 was positive. Since the patient still had active symptoms, favipiravir treatment was started. On the 7th day of hospitalization, the inflammatory response and symptoms completely regressed, and the patient was discharged.
Case 3 (admission: May 22, 2020)
A 2-year-old girl presented with fever for 8 days. Edema of the dorsum of hands and feet accompanied fever. Arthritis was present in the proximal interphalangeal joints of the hands and right knee. She did not have a conjunctival injection, skin rash, or changes in the lips and oral cavity. Other system examination was unremarkable. The parents were actively working physicians.
Laboratory tests were as follows: leukocyte count 18 × 103/µl, neutrophil count 8.24 × 103/µl, platelet count 626 × 103/µl, CRP 10.196 mg/dl (< 0.1), ESR 69 mm/h (0–20), procalcitonin 0.093 ng/ml (0–0.1). COVID-19 nasopharyngeal swab test results were negative. Bone marrow examination was normal.
The echocardiographic evaluation revealed increased perivascular echogenicity in the right coronary artery. IVIG and acetylsalicylic acid treatment were initiated with the diagnosis of incomplete KD. Then low-dose corticosteroid treatment was started. She recovered within 2 weeks. SARS-CoV-2 serology testing could not be performed.
Case 4 (admission: May 16, 2020)
A 2-year-old girl with a diagnosis of congenital adrenal hyperplasia presented with resistant fever for 6 days. She had bilateral conjunctival injection at the onset of symptoms and conglomerate lymphadenopathy in the right cervical region. Clinical examination revealed no signs of hepatosplenomegaly or lymphadenopathy in other lymphatic regions. She had no skin rash, no changes in the oral cavity, or in the extremities. Her father was a physician.
Laboratory examination revealed elevated acute phase reactants [CRP: 13.66 mg/dl (0–0.5), ESR 57 mm/h (0–20)], and increased leukocyte count (17.4 × 103/µl). The initial ECHO examination was normal. COVID-19 nasopharyngeal swab test results were negative, two times. After consultations with the Departments of Pediatric Hematology-Oncology, Infectious Disease, and Cardiology, antibiotic treatment was initiated for lymphadenitis.
At 2-week follow-up, the ECHO findings revealed an aneurysm in the left coronary artery. The SARS-CoV-2 serology was negative, either. IVIG, acetylsalicylic acid, and corticosteroid treatment were initiated with the diagnosis of incomplete KD.
Discussion
An increasing number of Kawasaki-like disease in patients with COVID-19 continue to be reported worldwide. We have reported four patients, along with the review of 320 pediatric patients from the systematic literature search (Table 1) [6, 12,13,14,15,16,17, 19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47]. In addition to these articles presented in the table, six articles reported Kawasaki-like disease in children with COVID-19 [36, 48,49,50,51,52]. These articles were not included since there were no details about the reported patients. In our study, the clinical features were consistent with incomplete KD in three patients. SARS-CoV-2 RT-PCR was negative in all except one while the serology was positive in one patient with negative RT-PCR. Corticosteroids, anakinra, IVIG, and acetylsalicylic acid were used in the treatment. Three patients recovered after the treatment while one patient died. Until today, 80 patients were reported from France, 17 patients from Italy, 132 patients from the USA, 74 patients from the UK, 3 patients from India, 12 patients from Spain, 1 patient from Israel, and 1 patient from Turkey. SARS-CoV-2 RT-PCR was negative in 120 (65.5%) of 183 patients while the serology was positive in 130 (83.8%) of 155 patients. The therapeutic options included IVIG, acetylsalicylic acid, tocilizumab, anakinra, enoxaparin, and methylprednisolone. All of the reported patients recovered after the treatment except one.
Hacettepe University is a tertiary reference center for Pediatric Rheumatology, and we serve a large population of children, probably serving as the reference center for a large geographic area in Turkey. IgA-vasculitis/Henoch-Schönlein purpura is the most frequent childhood vasculitis in our region. In our hospital where we diagnosed 129 (complete and incomplete) KD patients between June 2007 and September 2019 (incidence 0.8 per month), 3 patients were diagnosed with KD within a month during the COVID-19 pandemic. Although an approximately 3.7-fold increase in the incidence of KD was observed in our hospital during the pandemic, it was lower compared to reported incidences from other countries [6, 12]. For instance, in the series reported from Italy, a 30-fold increased incidence of Kawasaki-like disease was reported, and it is expected to reach similar figures in North America [12].
3 of our 4 patients had clinical features consistent with incomplete KD. Along with the incomplete clinical features, they had very high CRP, lactate dehydrogenase, and d-dimer levels, which were different from our classical KD patients. The reported prevalence of incomplete KD is 15 to 36.2% [53, 54]. In the literature review, incomplete KD phenotype was increased to 45.9% (n = 147). Thus, the rate of incomplete KD during the pandemic is higher compared to the pre-COVID-19 period. The rate could differ in different geographic areas. In our center in the pre-COVID period, Aydin et al. had reported the prevalence of incomplete KD of our center as 48.0% [55]. The rate increased to 75.0% (n = 3) in patients during the COVID-19 pandemic [55]. This finding suggests that we should maintain a high index of suspicion for incomplete KD in COVID-19 patients.
The underlying mechanisms of cardiovascular involvement in COVID-19 are currently unknown. However, Varga et al. reported that infected endothelial cells stimulate the inflammatory response and cause endotheliitis as a result of viral exposure [56]. Besides the viral effects, host factors are important in the pathogenesis of KD. Certain genetic or environmental factors may be suggested for the rather lower frequency of these cases in our center. First, the carrier frequency of MEFV mutations is high in our country, with a rate of 1/5 [57]. Asymptomatic heterozygous carriers of MEFV mutations have been indicated to have more frequent inflammatory symptoms, increased CRP, serum amyloid-A protein and the mRNAs for proinflammatory cytokines such as tumor necrosis factor, IL-1, IL-6 and IL-18 [58,59,60]. In one previous report, the authors also commented on a protective effect of MEFV variants against COVID-19 [58]. Such MEFV mutation carriers with subclinical inflammation may be protected against endemic infections due to the increased activity of the pyrin [60, 61]. A selective advantage against some pathogens such as Yersinia pestis in MEFV mutation carriers has recently been proposed [62]. The jury is out on whether FMF carriage might provide some protection against COVID-19 infection. Another issue is the possible protective effect of BCG vaccine [63]. BCG vaccine is included in the routine vaccination program in Turkey, and it is applied at two months of age. Previous studies have shown that the BCG vaccine protects against other viral infections by causing metabolic and epigenetic changes that increase the innate and trained immune response to infections [64]. Supporting this information, Arts et al. reported that BCG vaccination reduced yellow fever vaccine viremia by 71% [65]. On the other hand, the duration of the BCG effect remains uncertain. Long-term studies are needed with a broader analysis of monocyte function [65, 66]. However, the apparent lack of protection against COVID-19 was observed in the UK and France, where BCG vaccination was administered to older children [67]. It is hypothesized that when vaccination is done in the early infancy period, it may result in improved immune surveillance for lifelong, resulting in a milder viral disease. But if performed at an older age, this response may be short term or insufficient [67]. Finally, early measures such as curfews in children and travel restrictions might have an effect in reducing the spread of viruses and decreased incidence of KD.
We have not been able to show COVID-19 in two of our patients. Both parents of these two patients were actively practicing physicians at the time of the pandemics. RT-PCR-based assays performed on respiratory specimens were positive in 63 of 183 patients (34.5%) with KD and COVID-19. The sensitivity of RT-PCR tests is low, and it is affected by many external factors such as the sampling time, whether the sample is taken correctly, and the performance of the kits [68]. Ai et al. reported that 413 of 1014 (41%) RT-PCR test results of infected patients were negative at the initial presentation [69]. Although Waltuch et al. reported negative RT-PCR results of nasopharyngeal swab samples in four patients, serological tests of these patients were positive [25]. Serological tests have some advantages compared to RT-PCR tests such as presence of antibodies in the blood for a long time, unlike viral RNA, and stable structure of antibodies in sample processing steps. However, serological tests could be negative in the infected patients at an early stage of infection [70]. In our literature review, serologic tests were performed in 155 patients and 130 were positive (83.8%). The sensitivity of COVID-19 serology tests ranges from 72.7 to 100% [71].
Some children with COVID-19 developed a cytokine storm syndrome which may require intensive care [72]. Children with persistent fever, inflammation (neutrophilia, high CRP, and lymphopenia), and single or multi-organ dysfunction have been identified in the UK as “Pediatric Multisystem Inflammatory Syndrome in relation to SARSCoV-2 (PMIS-TS)” regardless of the SARS-CoV-2 RT-PCR test results [73]. This hyperinflammatory condition was named as “Multisystem Inflammatory Syndrome in Children (MIS-C)'' by the Centers for Disease Control and Prevention [74]. The phenotypes under this category are typical/atypical KD, Kawasaki shock syndrome, toxic shock syndrome, and macrophage activation syndrome/hemophagocytic lymphohistiocytosis [4]. In this study, we investigated only the group with typical/atypical KD accompanying COVID-19, to compare with our previous figures for KD: our first patient with incomplete KD also developed a hyperinflammatory syndrome.
During the COVID-19 pandemic, healthcare workers are worried about passing the infection to their families. The parents of two of our patients were healthcare workers who were at high risk to contact with infected patients. Similarly, healthcare workers were present in families of one every two patients in the study by Licciardi et al. [20]. Similarly, in early reports from China, 40 of 138 (29%) patients were healthcare professionals [75].
Conclusion
We present our patients with KD-like disease associated with SARS-CoV-2 infection. Since pediatric cases may come with findings consistent with atypical or incomplete KD, pediatricians need to be aware of such atypical presentations of COVID-19 infection for early diagnosis. A high clinical suspicion should be maintained for COVID-19-associated Kawasaki-like disease since it usually requires aggressive management. We await further studies to explain the clinical course of pediatric patients diagnosed with COVID-19 and KD, in particular, to clarify the pathophysiology. Whether there are geographic or ethnic factors affecting the occurrence of a Kawasaki-like disease in these patients will also be explained with further reports.
References
Bialek S, Gierke R, Hughes M, et al. Coronavirus Disease 2019 in Children—United States, February 12–April 2, 2020. MMWR. 2020;69(14):422. https://doi.org/10.15585/mmwr.mm6914e4.
Choi S-H, Kim HW, Kang J-M et al (2020) Epidemiology and clinical features of coronavirus disease 2019 in children. Clin Exp Pediatr 63(4):125. https://doi.org/10.3345/cep.2020.00535
Dong Y, Mo X, Hu Y et al (2020) Epidemiological characteristics of 2143 pediatric patients with 2019 coronavirus disease in China. J Emerg Med 58(4):712–713. https://doi.org/10.1016/j.jemermed.2020.04.006
Panupattanapong S, Brooks EB (2020) New spectrum of COVID-19 manifestations in children: Kawasaki-like syndrome and hyperinflammatory response. Cleve Clin J Med. https://doi.org/10.3949/ccjm.87a.ccc039
Gallo Marin B, Aghagoli G, Lavine K et al (2020) Predictors of COVID-19 severity: a literature review. Rev Med Virol. https://doi.org/10.1002/rmv.2146
Toubiana J, Poirault C, Corsia A, et al. Kawasaki-like multisystem inflammatory syndrome in children during the covid-19 pandemic in Paris, France: prospective observational study. 2020. https://doi.org/10.1136/bmj.m2094.
ECDC. Paediatric inflammatory multisystem syndrome and SARS-CoV-2 infection in children. 2020. https://www.ecdc.europa.eu/sites/default/files/documents/covid-19-risk-assessment-paediatric-inflammatory-multisystem-syndrome-15-May-2020.pdf
Chang L-Y, Lu C-Y, Shao P-L et al (2014) Viral infections associated with Kawasaki disease. JFMA 113(3):148–154. https://doi.org/10.1016/j.jfma.2013.12.008
Esper F, Shapiro ED, Weibel C et al (2005) Association between a novel human coronavirus and Kawasaki disease. JID 191(4):499–502. https://doi.org/10.1086/428291
Komatsu H, Fujisawa T (2008) Kawasaki disease and infection. Nihon Rinsho 66(2):278–282
Kikuta H, Sakiyama Y, Matsumoto S et al (1993) Detection of Epstein-Barr virus DNA in cardiac and aortic tissues from chronic, active Epstein-Barr virus infection associated with Kawasaki disease-like coronary artery aneurysms. J Pediatr 123(1):90–92. https://doi.org/10.1016/S0022-3476(05)81546-X
Verdoni L, Mazza A, Gervasoni A et al (2020) An outbreak of severe Kawasaki-like disease at the Italian epicentre of the SARS-CoV-2 epidemic: an observational cohort study. Lancet 395:1771–1778
Riphagen S, Gomez X, Gonzalez-Martinez C et al (2020) Hyperinflammatory shock in children during COVID-19 pandemic. Lancet 395(10237):1607–1608. https://doi.org/10.1016/S0140-6736(20)31103-X
Grimaud M, Starck J, Levy M et al (2020) Acute myocarditis and multisystem inflammatory emerging disease following SARS-CoV-2 infection in critically ill children. Ann Intensive Care 10(1):1–5. https://doi.org/10.1186/s13613-020-00690-8
Pouletty M, Borocco C, Ouldali N et al (2020) Pediatric multisystem inflammatory syndrome temporally associated with SARS-CoV-2 mimicking Kawasaki disease (Kawa-COVID-19): a multicentre cohort. Ann Rheum Dis 79:999–1006. https://doi.org/10.1136/annrheumdis-2020-217960
Feldstein LR, Rose EB, Horwitz SM et al (2020) Multisystem inflammatory syndrome in US children and adolescents. N Eng J Med 383(4):334–346. https://doi.org/10.1056/NEJMoa2021680
Davies P, Evans C, Kanthimathinathan HK et al (2020) Intensive care admissions of children with paediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) in the UK: a multicentre observational study. Lancet Child Adolesc Health 4(9):669–677. https://doi.org/10.1016/S2352-4642(20)30215-7
McCrindle BW, Rowley AH, Newburger JW et al (2017) Diagnosis, treatment, and long-term management of Kawasaki disease: a scientific statement for health professionals from the American Heart Association. Circulation 135(17):e927–e999. https://doi.org/10.1161/CIR.0000000000000484
Jones VG, Mills M, Suarez D (2020) COVID-19 and Kawasaki disease: novel virus and novel case. Hosp Pediatr 10(6):537–540. https://doi.org/10.1542/hpeds.2020-0123
Licciardi F, Pruccoli G, Denina M et al (2020) SARS-CoV-2-induced kawasaki-like hyperinflammatory syndrome: a novel COVID phenotype in Children. Pediatrics 146(2):e20201711. https://doi.org/10.1542/peds.2020-1711
Rivera-Figueroa E, Santos R, Simpson S et al (2020) Incomplete Kawasaki disease in a child with COVID-19. Indian Pediatr 57(7):680–681. https://doi.org/10.1007/s13312-020-1900-0
Deza Leon M, Redzepi A, McGrath E et al (2020) COVID-19 associated pediatric multi-system inflammatory Syndrome. JPIDS 9(3):407–408. https://doi.org/10.1093/jpids/piaa061
Labé P, Ly A, Sin C et al (2020) Erythema multiforme and Kawasaki disease associated with COVID-19 infection in children. J Eur Acad Dermatol Venereol. https://doi.org/10.1111/jdv.16666
Chiotos K, Bassiri H, Behrens EM et al (2020) Multisystem inflammatory syndrome in children during the COVID-19 pandemic: a case series. J Pediatric Infect Dis Soc 9(3):393–398. https://doi.org/10.1093/jpids/piaa069
Waltuch T, Gill P, Zinns LE et al (2020) Features of COVID-19 post-infectious cytokine release syndrome in children presenting to the emergency department. Am J Emerg Med. https://doi.org/10.1016/j.ajem.2020.05.058
Yozgat CY, Uzuner S, Duramaz BB et al (2020) Dermatological manifestation of pediatrics multisystem inflammatory syndrome associated with COVID-19 in a 3-year-old girl. Dermatol Ther. https://doi.org/10.1111/dth.13770
Rauf A, Vijayan A, John ST et al (2020) Multisystem inflammatory syndrome with features of atypical Kawasaki disease during COVID-19 pandemic. Indian J Pediatr. https://doi.org/10.1007/s12098-020-03357-1
Dasgupta K, Finch SE (2020) A case of pediatric multisystem inflammatory syndrome temporally associated with COVID-19 in South Dakota. SD Med 73(6):246–251
Whittaker E, Bamford A, Kenny J et al (2020) Clinical characteristics of 58 children with a pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2. JAMA 8:e2010369. https://doi.org/10.1001/jama.2020.10369
Greene AG, Saleh M, Roseman E et al (2020) Toxic shock-like syndrome and COVID-19: a case report of multisystem inflammatory syndrome in children (MIS-C). Am J Emerg Med. https://doi.org/10.1016/j.ajem.2020.05.117
Ferrero P, Piazza I, Bonino C et al (2020) Patterns of myocardial involvement in children during COVID-19 pandemic: Early experience from northern Italy. Ann Pediatr Cardiol 13(3):230. https://doi.org/10.4103/apc.APC_77_20
Ng KF, Kothari T, Bandi S et al (2020) COVID-19 multisystem inflammatory syndrome in three teenagers with confirmed SARS-CoV-2 infection. J Med Virol. https://doi.org/10.1002/jmv.26206
Ramcharan T, Nolan O, Lai CY et al (2020) Paediatric inflammatory multisystem syndrome: temporally associated with SARS-CoV-2 (PIMS-TS): cardiac features, management and short-term outcomes at a UK Tertiary Paediatric Hospital. Pediatr Cardiol 12:1–11. https://doi.org/10.1007/s00246-020-02391-2
Cheung EW, Zachariah P, Gorelik M et al (2020) Multisystem Inflammatory Syndrome Related to COVID-19 in previously healthy children and adolescents in New York City. JAMA 8:e2010374. https://doi.org/10.1001/jama.2020.10374
DeBiasi RL, Song X, Delaney M et al (2020) Severe COVID-19 in children and young adults in the Washington, DC metropolitan region. J Pediatr 223:199–203.e1. https://doi.org/10.1016/j.jpeds.2020.05.007
Capone CA, Subramony A, Sweberg T et al (2020) Characteristics, cardiac involvement, and outcomes of multisystem inflammatory disease of childhood (MIS-C) associated with SARS-CoV-2 infection. J Pediatr 224:141–145. https://doi.org/10.1016/j.jpeds.2020.06.044
Ouldali N, Pouletty M, Mariani P et al (2020) Emergence of Kawasaki disease related to SARS-CoV-2 infection in an epicentre of the French COVID-19 epidemic: a time-series analysis. Lancet Child Adolesc Health 4(9):662–668. https://doi.org/10.1016/S2352-4642(20)30175-9
Blondiaux E, Parisot P, Redheuil A et al (2020) Cardiac MRI of children with multisystem inflammatory syndrome (MIS-C) associated with COVID-19: case series. Radiology. https://doi.org/10.1148/radiol.2020202288
Perez-Toledo M, Faustini SE, Jossi SE et al (2020) Serology confirms SARS-CoV-2 infection in PCR-negative children presenting with Paediatric Inflammatory Multi-System Syndrome. MedRxiv. https://doi.org/10.1101/2020.06.05.20123117
Raut S, Roychowdhoury S, Bhakta S et al (2020) Incomplete Kawasaki disease as presentation of COVID-19 infection in an infant: a case report. J Trop Pediatr. https://doi.org/10.1093/tropej/fmaa047
Chiu JS, Lahoud-Rahme M, Schaffer D et al (2020) Kawasaki Disease features and myocarditis in a patient with COVID-19. Pediatr Cardiol 15:1–3. https://doi.org/10.1007/s00246-020-02393-0
Lee PY, Day-Lewis M, Henderson LA et al (2020) Distinct clinical and immunological features of SARS-COV-2-induced multisystem inflammatory syndrome in children. J Clin Invest 23:141113. https://doi.org/10.1172/JCI141113
Cazzaniga M, Baselli LA, Cimaz R et al (2020) SARS-COV-2 Infection and Kawasaki Disease: case report of a Hitherto Unrecognized Association. Front Pediatr 8:398. https://doi.org/10.3389/fped.2020.00398
Regev T, Antebi M, Eytan D et al (2020) Pediatric inflammatory multisystem syndrome with Central Nervous System Involvement and hypocomplementemia following SARS-COV-2 infection. Pediatr Infect Dis J 39(8):e206–e207. https://doi.org/10.1097/INF.0000000000002804
Gupta A, Gill A, Sharma M et al (2020) Multi-system inflammatory syndrome in a child mimicking Kawasaki disease. J Trop Pediatr. https://doi.org/10.1093/tropej/fmaa060
Pino R, Izurieta AC, Ríos-Barnés M et al (2020) Correspondence on: ‘Paediatric multisystem inflammatory syndrome temporally associated with SARS-CoV-2 mimicking Kawasaki disease (Kawa-COVID-19): a multicentre cohort’by Pouletty et al. Ann Rheum Dis. https://doi.org/10.1136/annrheumdis-2020-218538
Ouldali N, Pouletty M, Lokmer J et al (2020) Response to: ‘Correspondence on ‘Paediatric multisystem inflammatory syndrome temporally associated with SARS-CoV-2 mimicking Kawasaki disease (Kawa-COVID-19): a multicentre cohort’by Pouletty et al’by Pino et al. Ann Rheum Dis. https://doi.org/10.1136/annrheumdis-2020-218614
Dursun R, Temiz SA (2020) The Clinics of HHV-6 infection in COVID-19 pandemic: Pityriasis rosea and Kawasaki disease. Dermatol Ther. https://doi.org/10.1111/dth.13730
Belot A, Antona D, Renolleau S et al (2020) SARS-CoV-2-related paediatric inflammatory multisystem syndrome, an epidemiological study, France, 1 March to 17 May 2020. Euro Surveill 25(22):2001010. https://doi.org/10.2807/1560-7917.ES.2020.25.22.2001010
Iio K, Uda K, Hataya H et al (2020) Kawasaki disease or Kawasaki-like disease: influence of SARS-CoV-2 infections in Japan. Acta Paediatr. https://doi.org/10.1111/apa.15535
Moraleda C, Serna-Pascual M, Soriano-Arandes A et al (2020) Multi-inflammatory syndrome in children related to SARS-CoV-2 in Spain. Clin Infect Dis. https://doi.org/10.1093/cid/ciaa1042
Dufort EM, Koumans EH, Chow EJ et al (2020) Multisystem inflammatory syndrome in children in New York State. N Engl J Med 383(4):347–358. https://doi.org/10.1056/NEJMoa2021756
Jun HO, Yu JJ, Kang SY et al (2015) Diagnostic characteristics of supplemental laboratory criteria for incomplete Kawasaki disease in children with complete Kawasaki disease. Korean J Pediatr 58(10):369–373. https://doi.org/10.3345/kjp.2015.58.10.369
Sudo D, Monobe Y, Yashiro M et al (2012) Coronary artery lesions of incomplete Kawasaki disease: a nationwide survey in Japan. Eur J Pediatr 171(4):651–656. https://doi.org/10.1007/s00431-011-1630-3
Aydin EA, Ertugrul I, Bilginer Y et al (2019) The factors affecting the disease course in Kawasaki disease. Rheumatol Int 39(8):1343–1349. https://doi.org/10.1007/s00296-019-04336-2
Varga Z, Flammer AJ, Steiger P et al (2020) Endothelial cell infection and endotheliitis in COVID-19. Lancet 395(10234):1417–1418. https://doi.org/10.1016/S0140-6736(20)30937-5
Yilmaz E, Ozen S, Balcı B et al (2001) Mutation frequency of familial Mediterranean fever and evidence for a high carrier rate in the Turkish population. Eur J Hum Genet 9(7):553–555. https://doi.org/10.1038/sj.ejhg.5200674
Kavukçu S, Soylu A (2020) Could MEFV mutation carriage status have a protective role for COVID-19 pandemia? Med Hypotheses 144:109889. https://doi.org/10.1016/j.mehy.2020.109889
Lachmann H, Şengül B, Yavuzşen T et al (2006) Clinical and subclinical inflammation in patients with familial Mediterranean fever and in heterozygous carriers of MEFV mutations. Rheumatology 45(6):746–750. https://doi.org/10.1093/rheumatology/kei279
Kalyoncu M, Acar BC, Cakar N, Bakkaloglu A, Ozturk S, Dereli E, Tunca M, Kasapcopur O, Yalcinkaya F, Ozen S (2006) Are carriers for MEFV mutations" healthy"? Clin Exp Rheumatol 24(5 Suppl 42):S120–122
Schnappauf O, Chae JJ, Kastner DL et al (2019) The pyrin inflammasome in health and disease. Front Immunol 10:1745. https://doi.org/10.3389/fimmu.2019.01745
Manna R, Rigante D (2019) Familial mediterranean fever: assessing the overall clinical impact and formulating treatment plans. Mediterr J Hematol Infect Dis 11(1):e2019027. https://doi.org/10.4084/MJHID.2019.027
Batu ED, Özen S (2020) Implications of COVID-19 in pediatric rheumatology. Rheumatol Int 40(8):1193–1213. https://doi.org/10.1007/s00296-020-04612-6
Curtis N, Sparrow A, Ghebreyesus TA et al (2020) Considering BCG vaccination to reduce the impact of COVID-19. Lancet 395(10236):1545–1546. https://doi.org/10.1016/S0140-6736(20)31025-4
Arts RJ, Moorlag SJ, Novakovic B et al (2018) BCG vaccination protects against experimental viral infection in humans through the induction of cytokines associated with trained immunity. Cell Host Microbe 23(1):89–100. https://doi.org/10.1016/j.chom.2017.12.010(e105)
Pollard AJ, Finn A, Curtis N (2017) Non-specific effects of vaccines: plausible and potentially important, but implications uncertain. Arch Dis Child 102(11):1077–1081. https://doi.org/10.1136/archdischild-2015-310282
Escobar LE, Molina-Cruz A, Barillas-Mury C (2020) BCG vaccine protection from severe coronavirus disease 2019 (COVID-19). PNAS 117(30):17720–17726. https://doi.org/10.1073/pnas.2008410117
Younes N, Al-Sadeq DW, Al-Jighefee H et al (2020) Challenges in laboratory diagnosis of the novel coronavirus SARS-CoV-2. Viruses 12(6):582. https://doi.org/10.3390/v12060582
Ai T, Yang Z, Hou H et al (2020) Correlation of chest CT and RT-PCR testing in coronavirus disease 2019 (COVID-19) in China: a report of 1014 cases. Radiology 296(2):E32–E40. https://doi.org/10.1148/radiol.2020200642
Lauer SA, Grantz KH, Bi Q et al (2020) The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: estimation and application. Ann Intern Med 172(9):577–582. https://doi.org/10.7326/M20-0504
Wikramaratna P, Paton RS, Ghafari M (2020) Estimating false-negative detection rate of SARS-CoV-2 by RT-PCR. MedRxiv. https://doi.org/10.1101/2020.04.05.20053355
Hennon TR, Penque MD, Abdul-Aziz R et al (2020) COVID-19 associated multisystem inflammatory syndrome in children (MIS-C) guidelines; a Western New York approach. Prog Pediatr Cardiol 57:101232. https://doi.org/10.1016/j.ppedcard.2020.101232
Health RCoPaC (2020) Guidance: paediatric multisystem infl ammatory syndrome temporally associated with COVID-19. https://www.rcpch.ac.uk/sites/default/files/2020-05/COVID-19-Paediatric-multisystem-%2520inflammatory%2520syndrome-20200501.pdf
Prevention. CfDCa (2020) Multisystem INFL ammatory syndrome in children (MIS-C) associated with coronavirus disease 2019 (COVID-19). CDC Health Alert Network publication CDCHAN-00432. https://emergency.cdc.gov/han/2020/han00432.asp
Wang D, Hu B, Hu C et al (2020) Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan. China JAMA 323(11):1061–1069. https://doi.org/10.1001/jama.2020.1585
Funding
No external funding for this manuscript.
Ethics declarations
Conflict of interest
The authors have indicated that they do not have any financial and non-financial potential conflicts of interest to disclose.
Informed consent
Written informed consent was obtained from the presented patients and their parents.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article
Cite this article
Akca, U.K., Kesici, S., Ozsurekci, Y. et al. Kawasaki-like disease in children with COVID-19. Rheumatol Int 40, 2105–2115 (2020). https://doi.org/10.1007/s00296-020-04701-6
Received:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1007/s00296-020-04701-6
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
Keywords
Profiles
- Yasemin Ozsurekci View author profile
- Ezgi Deniz Batu View author profile
- Selcan Demir View author profile
- Seza Ozen View author profile